
SUTURING
- Nov 21, 2025
- 4 min read
Tavishi
College continues to go swimmingly! I've started to run into the issue of having too many events I want to go to and too little time. Thankfully, I have time management skills (I CAN do everything I just need to lock in!!!!).

Jokes aside, I did have to skip a suturing practical with the Surgical Society that I REALLY wanted to go to...
I did, however, do all the pre-reading beforehand (I cannot help but read about whatever I'm about to do before I go in.)
I thought I might as well indulge my knot-tying dreams with a Kradigan though! (I just want to yap.) Anyways, I'm not super sure how all this information compares to regular human medicine, and because it's surgical techniques, I highly doubt it's all up to date because surgical techniques are always evolving.
Suturing is used to close incisions; either intentionally made ones, or accidentally made ones. If suturing is used on accidentally-created-incisions (see: deep gashes and scrapes), it's because wounds are too deep to heal on their own well. Once, I decided to make an incision on my chin. Unfortunately, I did this by blunt force trauma on ice, and not with a scalpel. I got stitches and a cool scar on my chin!!

Suturing is really just sewing a wound shut, and can be either absorbable or non-absorbable. Non-absorbable stitches require removal later on, which is time-consuming and invasive; hence the invention of absorbable sutures. Non-absorbable sutures are generally a lot stronger than absorbable sutures, and are oft used in external wounds or incisions that require a lot of healing time because of their aforementioned tensile strength. Absorbable sutures are preferred when closing incisions that can't really have stitches removed later on because of how invasive that procedure is, or when less of a scar is wanted. Absorbable sutures are also absorbed by phagocytosis or proteolytic measures or by hydrolysis (breakdown by cellular enzymes or by water).
Nonabsorbable suture materials can be metallic or fabric. Commonly used nonabsorbable suture materials include nylon, polypropylene, and polymerized capractolam. Nylon is either braided multifilaments or one monofilament, with high tensile strength, but does give out after about six months. Nylon is commonly used in skin sutures, especially in swollen skin. Polypropylene is only available in monofilaments, and is commonly used in cardiovascular sutures. Polymerized capractolam is only a twisted multifilament (think twizzler), but is very strong, but can cause a lot of foreign body reaction, and so it's most commonly used only in skin wounds.

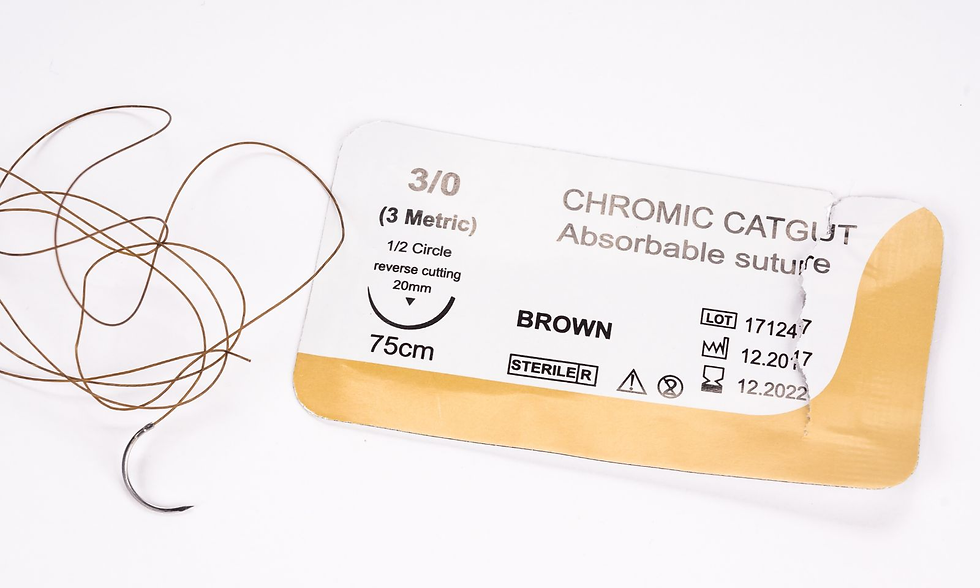
Absorbable sutures generally have less tensile strength, and give out after about 60 days. Common absorbable suture materials include catgut, polyglactin 910, and poliglecaprone. Catgut is, of these, the only natural material. Ironically, catgut is in fact not composed of cat stomach, but sheep or cow intestinal submucosa. Catgut is absorbed fairly quickly compared to other suture materials, and is a multifilament. Polyglactin 910 is a synthetic braided multifilament suture material, and is often used in oral surgery. It degrades fully within about 70 days. Poliglecaprone is a synthetic monofilament, and of all mentioned absorbed suture materials, lasts the longest prior to degradation. It causes minimal inflammation and reaction within tissue.

When choosing suture materials, a few things are to be considered. For one, slow-healing tissue should be sutured with non-absorbable tissue. For example, wounds in the fascia or tendons. In the bladder or any tissue where stones can form, sutures can accidentally attract and create lithiasis (fancy words for.. having bladder stones etc.) So, quickly absorbing sutures are preferred.

Monofilament sutures are preferred in the case of infected or contaminated tissue, as multifilament is more likely to get infected. Similarly, natural suture material like catgut or silk is to be avoided. Sepsis is bad.
I should care about suture needles. I don't. Moving on to the fun stuff.. knots!
Just like when sewing clothes, you want to make the seam as invisible as possible. This means tying tiny knots that are close to the skin. You don't want it to tight, or the fabric (skin) will bunch up, and you get a nasty scar. You don't want to do it too loose, either. If it's not evenly spaced out, it'll also affect how the fabric looks. The sort of goal in both sewing and suturing (especially on the skin), is not to create ripples on the surface while also keeping everything in its place.
When you think of the first step of tying your shoelaces, that is a simple throw. That throw can be used in several combinations to make a variety of more complex knots.
For example, a very well used, the square knot.
Unlike in sewing, you're not holding the needle with your fingers; rather, you're using something like forceps called a needle driver. The position of the needle driver, thus, is very important to knot tying.
When tying a square knot, you start with one simple throw followed by another. During this, it's crucial that the needle driver sandwiched between both strands.

If, during the second throw, your needle driver is outside of the strands, you accidentally make a granny knot, which is a weaker version of the square knot and is generally not intentional.
If you want to make an even stronger square knot, you pass the second thread an extra time through the loop during the first throw, and proceed with the second throw as normal, producing a surgical knot.

If you mess up when tightening the knot, or when placing the second throw (you have to switch directions!) you accidentally make a sliding knot, which is, again, not the intent.

Again, I am no surgeon and definitely no medical expert, so take this all with a grain of salt. I've definitely left out a lot of important stuff (like suture patterns and needles), but this is just some of the stuff that piqued my interest when I was studying!
Okay, enjoy!



Comments